
In their quest for a “slimmer waist,” people often focus on fat tissue: diet, exercise, liposuction…
However, in some bodies, the problem is not fat, but the architecture and angles of the rib cage.
Therefore, when the goal of “waist narrowing” is limited to soft-tissue procedures, the results
are either insufficient or unsustainable.
What makes Ribella different is that it is not just a “procedure,” but a medically structured system
centered on scarless rib remodeling / ultrasound-guided rib
remodeling: hospital safety, pain management, 3D planning, personalized biomechanical stabilization
corset, insurance, and follow-up protocol…
This article provides a scientific framework to answer a single question: Why is rib reshaping not an
area that can be performed on an outpatient basis in the plastic surgeon’s clinical setting, but rather an
area that requires the infrastructure of thoracic surgery in terms of anatomy, respiratory physiology,
and complication management?
1) The rib is not an “ordinary bone”: It is an active part of respiratory biomechanics. Ribs, together
with the spine, sternum, costochondral junction, and diaphragm, form the dynamic skeleton of the
thorax. The chest cage changes volume during breathing, works in coordination with diaphragm
movement, and is intertwined with neurovascular structures through the intercostal spaces.
Therefore, the “rib remodeling” approach is not just about “shaping”:
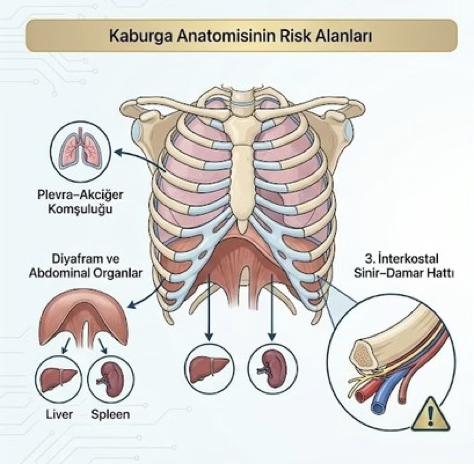
- Understanding rib cage anatomy
- Knowing the diaphragm’s proximity
- Managing the pleura-lung relationship
- Protecting the intercostal nerve-vascular bundle
- Being able to immediately intervene in case of a thoracic complication, if necessary.
Scarless Rib Remodeling – Ribella Technique: Why
a Thoracic Surgeon?
This is the point Ribella particularly emphasizes: the method is not a cosmetic “shortcut”; it is
a rib reshaping system based on anatomical precision + clinical safety.
2) Who handles “rib fractures in the emergency room”? The logic is the same.

In daily practice, when there is a serious problem
with the ribs (trauma, suspected pneumothorax,
hemothorax, risk of intrathoracic injury), the team
managing the patient has a “thoracic surgery”
reflex. This is because the ribs cannot be treated
like an orthopedic bone due to their proximity to
internal organs.
The same reflex applies to aesthetic rib remodeling at this point:
If you are working on the ribs, the specialty that knows the thorax and complication
management comes to the fore.
3) “Surgeon-fee only” model: Hidden risk, hidden cost While some techniques in the market
appear to be “expensive,” they are often based on the following model:
The majority of the fee is the surgeon’s fee.
- The procedure is mostly performed in outpatient clinic conditions
- Discharge to hotel on the same day
- The procedure is mostly performed in outpatient clinic conditions
- Discharge to hotel on the same day
- No/limited hospitalization
- Pain management (e.g., cryo) absent or unclear
- No planning (3D simulation)
- No brace or extra fee
- Follow-up program not structured
- No insurance
This table leads to the following conclusion: a procedure that appears “expensive on the label”
may in fact be worthless because it does not include the full system cost and safety
layers. Ribella’s comparative articles explain this
distinction precisely: it is not the price that should be compared, but the “clinical content of the
package.
4) Ribella “Full-System” approach: Hospital security + protocol + outcome stabilization

4.1 JCI-accredited hospital infrastructure Ribella does not perform the procedure as an
“outpatient clinic”; it is performed in a JCI-accredited hospital setting with the safety infrastructure
of anesthesia and intensive care.
This is not merely a matter of “comfort”; it is a standard for managing the risk of complications.
The ribs are a “highly sensitive” area in terms of pain; due to the intercostal
nerve pathway,
postoperative pain management is critically important.
In the Ribella system, intercostal nerve cryoablation/cryoanalgesia is
described as a protocol that “does not leave pain to chance”: an approach
that reduces the need for opioids/narcotics and facilitates early mobilization.
This is one of the strongest clinical advantages that a thoracic surgeon, who
has been using this area in thoracic surgery for years, has brought to
aesthetic rib remodeling.
4.2 Cryoanalgesia (cryoablation): Rib pain should be managed scientifically

4.3 3D Anatomical Planning, Golden Ratio Analysis, and Custom Biomechanical Stabilization
The most critical stage of rib remodeling
procedures is not the surgery itself, but the
planning.
This is because changing the rib angle is
technically
possible; however, achieving the correct aesthetic
ratio, correcting asymmetries, and
permanently stabilizing the result requires
advanced anatomical
planning.
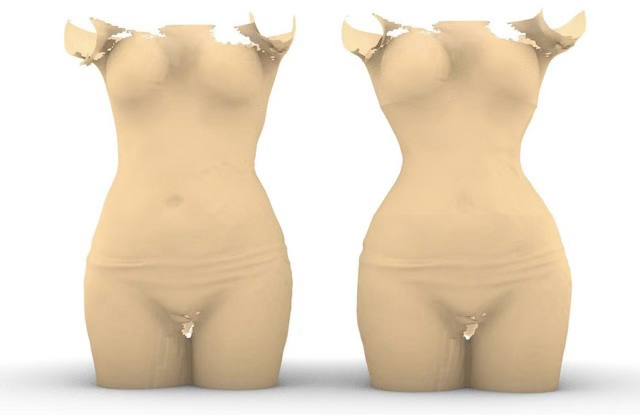
3D Body Surface Scan + Skeletal CT Integration
The patient’s body is modeled in three dimensions using a high-resolution 3D body scan.
- At the same time, three-dimensional anatomical data of the skeletal system is obtained using a
thoracic CT scan. - By integrating soft tissue and bone data, the patient’s complete anatomical model is created at both
the surface and skeletal levels.
This stage is a critical point of differentiation.
Many rib contouring approaches rely solely on superficial measurements; however, the true aesthetic
form cannot be determined without evaluating the
rib angle + spinal curvature + chest rotation together.

Golden Ratio-Based Digital Design
The obtained 3D data is analyzed according to the “golden ratio” parameters compiled from aesthetic
perception studies conducted in different cultures around the world.
These parameters include:
- Waist–Hip Ratio
- Waist–Chest Ratio
- Waist–Breast Ratio
- Breast–Hip Ratio
- Waist–Neck Proportion * Body Fat Distribution Balance
There are many aesthetic reference values such as these.
The patient’s skeletal structure is simulated in a computer environment according to these golden ratio
parameters,
and an optimal aesthetic model is created.
However, this model is not mandatory
Patient-Involved Aesthetic Decision-Making Mechanism

Simulation images:
Are shown to the patient before surgery via AR glasses or
- On a high-resolution screen.
At this stage, the patient may: - Find the golden ratio more natural,
- Request a more minimal slimming,
- Demand a more dramatic “barbie waist,”
- Or may not want the aesthetic change to be very noticeable.
The decision is not unilateral.
The final form is determined by: - The breast surgeon from a health perspective,
- The patient from an aesthetic expectation perspective,
- The engineering team from a technical feasibility perspective…
- It is determined by mutual agreement among the engineering team in terms of technical
feasibility.
This multidisciplinary decision model is one of the fundamental security layers of the Ribella
system.
Asymmetry Analysis and Correction

Thoracic asymmetries that go unnoticed in many patients
are present:
- Trunk rotation due to scoliosis
- One rib being more prominent than the other
- Congenital or developmental rib flare differences
- Optical waist asymmetry due to spinal curvature
This is why chest CT is routinely requested.
With this data: - Right–left rib volume is compared
- Rib angles are measured
- Rotational deformities are analyzed
Asymmetries are corrected in the digital environment and a symmetrical aesthetic goal is set.
Thanks to this technology, the goal is not only slimming but also a symmetrical and balanced
chest architecture.

Custom-Made 3D Biomechanical Corset
After planning is complete, the process does not end with surgery alone.
In accordance with the form approved in the simulation:
- A custom-made Ribella corset,
- Produced with a 3D printer,
- Providing biomechanical stabilization, is manufactured. This corset:
- It is not an ordinary medical corset.
- It provides stabilization during the healing process of the newly created rib angle.
- It maintains the corrected asymmetry.
- It biomechanically supports the preservation of the result.
This is where the Ribella system’s “result security” comes into play
Because in many rib reshaping techniques:
- There is no prior simulation,
- There is no guarantee of asymmetry correction,
- There is no stabilization system,
- The result cannot be seen by the patient before surgery.
The fundamental difference with Ribella is this:
The result is checked before surgery.
It is approved if satisfactory. And it is biomechanically preserved. In aesthetic surgery, being
able to see the result in advance and make a decision about it is the highest level of control
mechanism in terms of patient safety.
4.4 Anatomical Scope and Safe Shaping Up to the 7th Rib
The most important technical limitation in rib remodeling literature is anatomical depth. Many
alternative techniques:
- Works more superficially
- Remains limited to the lower ribs
- Cannot progress beyond the 7th rib
The main reason for this is that the 7th rib level requires advanced knowledge of thoracic anatomy due to:

Proximity to the diaphragm
- Proximity to the pleural border
- Density of intercostal neurovascular structures.
Specialties other than thoracic surgery generally do
not reach this level due to technical and safety concerns.
In the Ribella system, however: - Nearly 20 years of thoracic surgery experience
- Thousands of rib fractures
- Chest wall deformity surgeries
- Rib tumor resections
Anatomical mastery gained from such experience allows for controlled reshaping up to the
7th rib.

This broad anatomical coverage area provides:
- A more natural hourglass shape
- Waist narrowing not only in the lower segment but also in the upper segment
- A more homogeneous thoracic curve
- A more feminine and anatomical transition Therefore, Ribella is defined not only as “slimming”
but as a rebalancing of the thoracic architecture.
Clinical Setting vs. Hospital Security
Some applications:
- In a clinical setting
- Same-day discharge
- Without postoperative hospital stays performed.
Ribella is administered: - In a JCI-accredited hospital
- With a 2-night hospitalization
- Using a structured pain protocol
- With complication insurance
- With a long-term follow-up plan.
This difference is not just a matter of comfort, but of risk management.
5) Complication Management: “Who will intervene, where, and how quickly?”
Procedures such as rib remodeling / percutaneous
rib reshaping / ultrasound-guided rib remodeling are
not harmless just because they are “incision-free.”
This is because the working area here is the rib
architecture, and the ribs:
- Are located adjacent to the pleura and lungs
- Are anatomically close to the diaphragm and
abdominal organs - Each rib has an intercostal nerve–vascular bundle
beneath it
Therefore, rib contouring, unlike conventional “soft tissue body contouring” procedures, requires an
expert who is knowledgeable about thoracic pathophysiology and thoracic complication algorithms
in the event of a potential problem.
5.1 “Why does a plastic surgeon need a breast surgeon?” It must be clearly stated: Plastic
surgery is not a specialty based on training in internal organ surgery and thoracic complication
management. During a procedure performed in the thoracic region, such as rib remodeling:
Suspected pleural irritation/pneumothorax
- Unexpected respiratory-related condition
- Management of chest wall bleeding/hematoma
- Assessment of intrathoracic risks
When scenarios such as these arise, the answer to the question “who should be called?” is clear in
practice: thoracic surgery.
In other words, in some models, the following actually occurs:
The person performing the procedure needs someone who can manage the thorax in the event of a
complication.
This is where Ribella’s fundamental argument begins: An intervention involving the thorax should
be performed by a specialty that thinks in terms of the thorax and
can manage complications. This is not merely a matter of “title”; it is a clinical necessity for
patient safety.
5.2 The “hidden risk” of the same-day model in a clinical setting The weakest link in
some alternative techniques is this: The procedure is performed and the patient is sent to
a hotel the same day. This approach poses two critical risks for the patient:
- In the event of a problem that may develop in the early stages, the patient remains in their hotel
room instead of with the “clinical team.” - If the necessary imaging/monitoring/intervention chain is not set up in the same structure, the
patient is referred to the emergency room with a delay, and the process spirals out of control.
Therefore, the “surgeon-fee only” model is fragile not only financially but also in terms of
organizational security.

5.3 What sets Ribella apart:
Positioning the procedure as a “hospital protocol” What distinguishes Ribella from its competitors
is that it turns the procedure into a complete medical protocol:
- The operation is performed in a JCI-accredited hospital
- Early-stage safety monitoring with 2 nights of hospitalization
- English medical summary + fit-to-fly documents upon discharge
- Structured follow-up plan at 2 months and 6 months
- Cryotherapy/cryoanalgesia protocol
- Customized biomechanical corset system This is not marketing; it is risk management.
5.4 Complication and travel insurance The biggest fear for international patients:
“If something goes wrong, what will happen when I return to my country?”
Ribella offers the Travel and Treatment Assurance Insurance system here.
This system:
- Secures the process in case of complications
- Provides support for health/logistical issues that may arise during travel
- Offers transfer and organizational support when needed
Most competitors leave a gap here.
5.5 The most expensive thing is poorly managed risk
Ribella, however, systematizes the process.
The real cost is not the price. The real cost is:
- Not being able to access the right department in case of complications
- Managing a crisis without hospital infrastructure
- Being left alone upon returning to your country
If you touch the ribs, you must know the thorax.
6) The Core Difference Compared to Surface-Focused Approaches Like RibXcar,
RibSculpt, and Rib Mold Today, techniques such as RibXcar, RibSculpt, Rib Mold, and
similar ones are applied in the field of rib contouring.
However, the critical question is:
At what anatomical depth is the shaping performed?
The rib is not just a bone that determines the external appearance.
Thoracic architecture must be evaluated in conjunction with respiratory dynamics,
diaphragm relationship, intercostal neurovascular structures, and chest cage geometry.
The safety and durability of a rib remodeling method depend on the answers to the following
questions:
- Up to which rib level is it safe to work?
Ribella is not just rib contouring. Ribella is a rib architecture remodeling approach. - Is planning based on surface measurements, or is CT-supported 3D analysis performed?
- Is pain management carried out according to the thoracic surgery protocol?
- Is the procedure performed in a clinical setting, or in a JCI-accredited hospital?
- Is there a capacity for intra-thoracic intervention if complications arise?
- Is there an insurance and follow-up system in place for international patients?
Ribella is not just rib contouring. Ribella is a rib architecture remodeling approach.
It is based on Planning + Implementation + Pain Management + Stabilization + Hospital Safety +
Insurance Chain.
If any link in this chain is missing, the result remains merely an aesthetic intervention.
7) Technical Terminology
Target word sets:
- scarless rib remodeling
- ultrasound-guided rib remodeling
- percutaneous rib reshaping
- monocortical rib osteoclasis
- rib contouring / rib angle remodeling
- hourglass waist / waist narrowing surgery
- rib flare correction
- 3D simulation / 3D-printed custom corset
- cryoanalgesia / cryoablation intercostal nerves
- JCI-accredited hospital rib contouring
- complication insurance / travel & treatment assurance
8) Frequently Asked Questions (FAQ)
Is Ribella a rib removal surgery?
No. Instead of removing ribs, Ribella involves repositioning the rib angle using micro-entry and
stabilizing it.
Why a thoracic surgeon rather than a plastic surgeon?
Because the ribs are part of the thoracic structure, and managing complications falls
within the field of thoracic surgery.
Will there be pain?
Cryoanalgesia is used to control postoperative pain.
How is the result guaranteed?
It is stabilized with 3D simulation + a personalized biomechanical corset.
What is the most critical difference in terms of safety?
JCI-accredited hospital + insurance + structured follow-up.
Conclusion Rib reshaping is not only aesthetic, but also involves intervention in thoracic
anatomy.
Therefore:
- It is rational for it to be performed by a thoracic surgeon who:
- Knows anatomy
- Can manage complications
- Controls pain scientifically
- Plans and stabilizes the outcome
- Works in a safe hospital environment
Is it not important to you to see and control the outcome before surgery, to know that
asymmetries will be corrected, and to see that it will be biomechanically stabilized?
This content is for informational purposes only. Suitability is determined by examination and
personal evaluation